
More Information
Submitted: May 08, 2026 | Accepted: May 15, 2026 | Published: May 18, 2026
Citation: Rehman FU, Rahman N, Abbas M, Siddiqui YS. Punctate Tarsus with Deformed Foot – A Rare Presentation of Chondrodysplasia punctata. Arch Clin Exp Orthop. 2026; 10(1): 6-8. Available from:
https://dx.doi.org/10.29328/journal.aceo.1001024
DOI: 10.29328/journal.aceo.1001024
Copyright Licence: © 2026 Rehman FU, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Punctate Tarsus with Deformed Foot – A Rare Presentation of Chondrodysplasia punctata
Fazal Ur Rehman1, Nusra Rahman1, Mazhar Abbas2 and Yasir Salam Siddiqui2
1Department of Anatomy, J.N. Medical College, Faculty of Medicine, A.M.U., Aligarh, India
2Department of Orthopaedic Surgery, J.N. Medical College, Faculty of Medicine, A.M.U., Aligarh, India
*Corresponding author: Dr. Yasir Salam Siddiqui, Assistant Professor, Department of Orthopaedic Surgery, J.N. Medical College, Faculty of Medicine, A.M.U, Aligarh, Email: [email protected]
Chondrodysplasia punctata is a heterogeneous group of skeletal dysplasias characterized by punctate epiphyses. The spectrum of the disease ranges from incidental findings to severe disabilities, including skeletal deformities, respiratory insufficiency and multisystem complications increasing the risk of early mortality. Clinico-radiologically it presents as disproportionate dwarfism, joint contracture and punctate calcifications visible in the epiphyses. This entity is extremely rare and the diagnostic challenge is posed by clinical manifestations and image resemblance to various pathologies including warfarin embryopathy and other skeletal dysplasias characterized by epiphyseal stippling. At present, the literature highlights a considerable gap in awareness about this condition. Therefore, we are presenting a 15 months old male child with Chondrodysplasia punctata detected incidentally, who presented to our paediatric orthopaedic OPD with bilateral punctate tarsus with right deformed foot.
Chondrodysplasia punctata is a heterogeneous group of skeletal dysplasias characterized by atypical calcifications (punctate epiphyses or stippled epiphyses) in the cartilage during foetal and neonatal development [1]. Even though its exact incidence varies, it affects both males and females, with manifestations visible as early as the prenatal period or at birth [2]. Chondrodysplasia punctata is often associated with defects in endochondral ossification, often linked to abnormalities in specific metabolic pathways [3,4]. The spectrum of the disease ranges from incidental findings to severe disabilities, including skeletal deformities, respiratory insufficiency and multisystem complications that increases the risk of early mortality [4,5]. Clinico-radiologically it presents as disproportionate dwarfism, joint contracture and punctate calcifications visible in the epiphyses. Involvement of the cardiac and respiratory system has also been described in literature [5,6]. This entity is extremely rare, and the diagnostic challenge is posed by clinical manifestations and image resemblance to various pathologies including warfarin embryopathy and other skeletal dysplasias characterized by epiphyseal stippling [4-6].
At present, the literature highlights a considerable gap in awareness about this condition. Therefore, we are presenting a 15-month-old male child with Chondrodysplasia punctata detected incidentally, who presented to our paediatric orthopaedic OPD with bilateral punctate tarsus with a right foot deformity.
A 15 months old male child was brought to our paediatric orthopaedic OPD with complaints of deformity of right foot since birth. The patient was their second child with one male sibling without any such complaints. There was no history of consanguinity among the parents. The parents also added that there was no developmental delay and any systemic illnesses in the child except for the right deformed foot. The baby was full-term, delivered through vaginal route. There was no history suggestive of any maternal infection or any exposure to teratogenic agents throughout the antenatal period. There was no family history of congenital deformity of feet or any other joint deformity.
Clinical examination revealed that the right foot was in attitude of valgus with contracture at the ankle. The other foot was normal. There were no other skeletal abnormalities. Furthermore, no definite syndromic features were noted. Systemic examination including cardiovascular system, central nervous system, respiratory system, abdomen and genitalia was unremarkable. There was also no involvement of the skin over the extremities and trunk. Ocular examination was also within normal limits. Ultrasonography of abdomen and echocardiography were also within normal limits. Radiological skeletal survey revealed punctate stippled calcification of bilateral tarsal bones (Figures 1,2), with oblique orientation of talus on right side as compared to left one. Both radiographs showed normal epiphyses around the knee joint. The rest of the skeletal survey was normal. A clinico-radiological diagnosis of Chondrodysplasia punctata with right sided oblique talus was made and the child was put on serial manipulation with casting. The other investigations including specific lab investigations and genetic studies were not done due to financial constraints and resource-limited setting. The child responded well to the treatment, and gradually deformity corrected and the parents were communicated about the need of regular follow-up for proper treatment, rehabilitation and to monitor progression of the disease, if any.
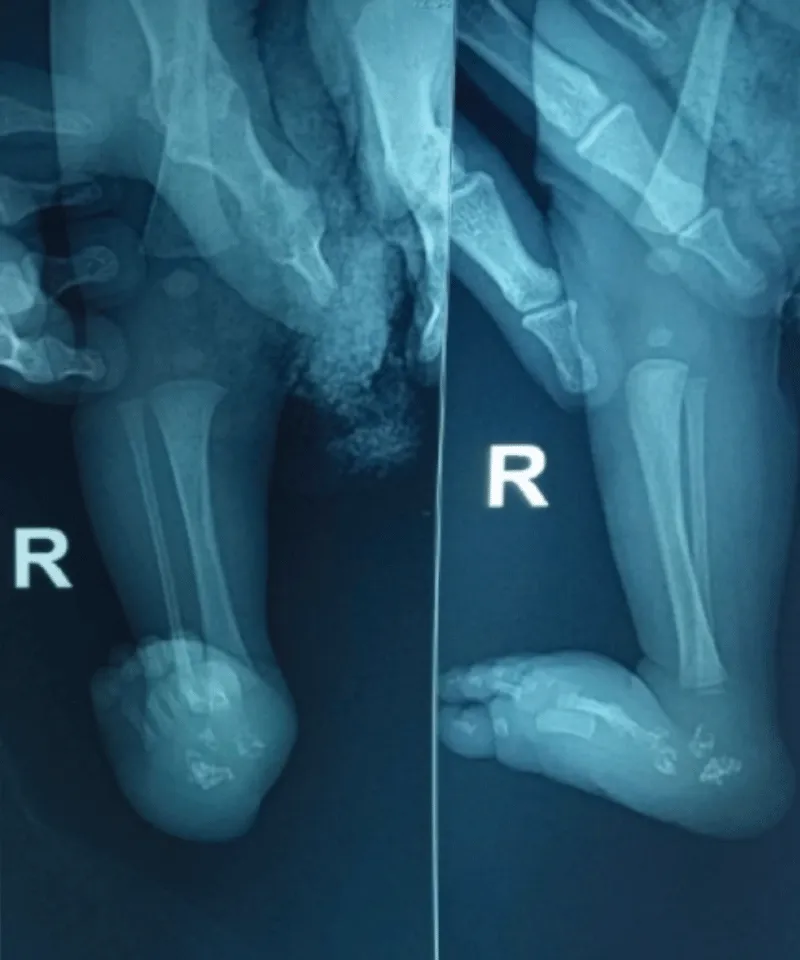
Figure 1: AP and lateral radiograph of the right leg including foot showing valgus alignment of foot with oblique orientation of talus with punctate stippling of tarsal bones, suggesting Chondrodysplasia punctata. Also note normal epiphyses around the knee joint.
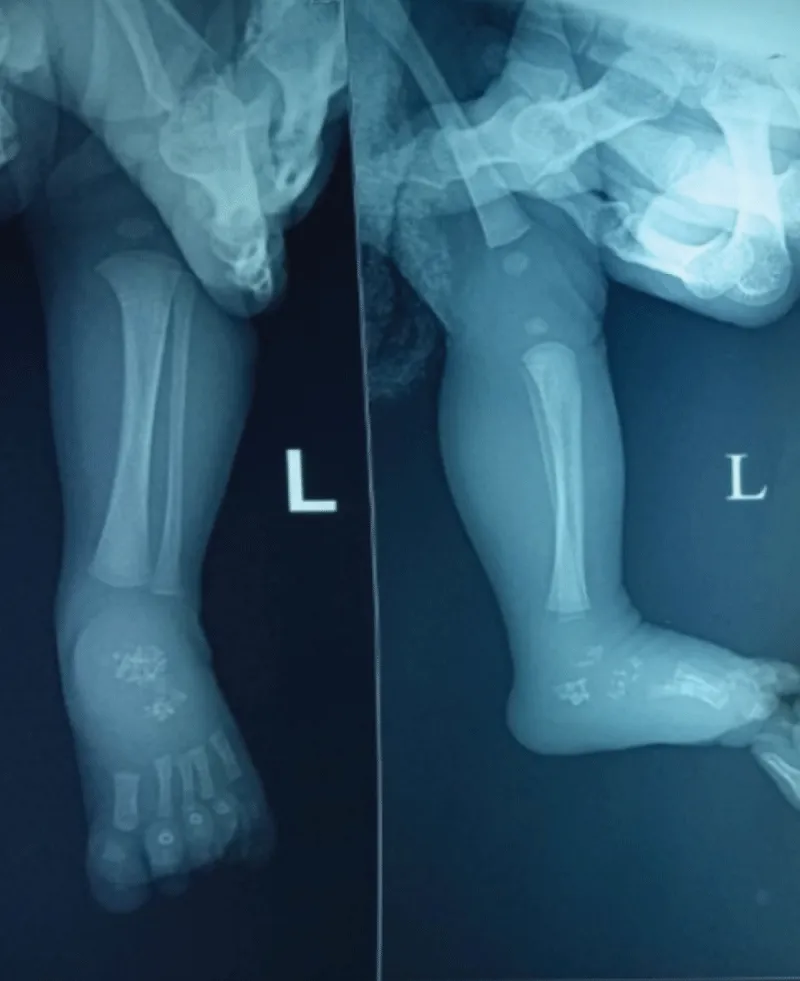
Figure 2: AP and lateral radiograph of the left leg including foot showing normal foot and ankle alignment with punctate stippling of tarsal bones, suggesting Chondrodysplasia punctata. Also note normal epiphyses around the knee joint.
Chondrodysplasia punctata is an exceptionally rare entity and is associated with bone remodeling defect which significantly affects muscles, tendons and ligaments leading to joint stiffness and contractures [7]. Clinical features are usually apparent at birth, but disease severity may vary among the patients. Diagnosis is based on clinico-radiological features and biochemical findings [6].
The literature describes the pathogenesis as a wide range of abnormal genetic and metabolic conditions presenting as variable overlapping clinical manifestations and image resemblance to various pathologies including warfarin embryopathy and other skeletal dysplasias characterized by punctate epiphyses [5-8]. The literature is limited to isolated case reports, without a clear pathogenic mechanism explaining the association. Some authors have suggested that the occurrence may be incidental (as in our case), while others have speculated about shared developmental pathways contributing to skeletal abnormalities.
Classical rhizomelic or X-linked forms present with symmetrical shortening of the proximal long bones, extensive punctate calcifications in the cartilage (stippled epiphyses) and abnormal vertebral development, while the atypical cases presents with asymmetric localized punctate stippling. The prognosis is poor in classical form when compared to atypical ones. The isolated involvement of foot deformity as in our patient is a rare phenotypic expression of the disease, without disproportionate dwarfism and dysmorphic facial distinctiveness. Recognizing this unusual association is important for clinicians and radiologists for further work up to rule out the other organ systems involvement [6,8]. Molecular testing does provide a definitive diagnosis, however radiologic evaluation remains a cornerstone in identifying and characterizing these entities, especially when genetic testing is unavailable. Other than plain radiographs, advanced imaging modalities (ultrasound and computed tomography) are critical to confirm the presence of punctate epiphyses, to assess the severity of skeletal abnormalities and to exclude other differential diagnoses such as other skeletal dysplasias [2,9,10]. Treatment is not definitive and requires multidisciplinary approach, for symptomatic and supportive care [5,6,10].
Strengths and limitations
Our case study highlights the fundamental role of plain radiographs in diagnosing Chondrodysplasia punctata, predominantly in atypical presentations and thus contributes to the understanding of phenotypic inconsistency and radiologic presentation of the disorder. Although our case presents an unusual phenotypic manifestation of Chondrodysplasia punctata, particularly due to an isolated foot involvement, however, it remains demanding to be in agreement on whether this phenotype represents a rare manifestation of an established subtype or a potentially distinct variant of the disorder, this represents a limitation of our study, especially in absence of molecular or biochemical confirmation of the disease. We do agree due to financial constraints, we were not able to precisely classify the subtype and thus predict the prognosis.
Chondrodysplasia punctata is a rare skeletal dysplasia that presents diagnostic and therapeutic challenge. The limited literature along with the variable phenotypic expression of the disease with overlapping clinico-radiological features with other conditions makes early recognition difficult, especially in subtle cases. Clinical features are usually perceptible at birth, but magnitude of the disease may be diverse among the patients. Diagnosis is based on clinico-radiological features and biochemical findings. The present case is unique and require worth reporting, that there was only foot involvement without typical skin or ocular involvement. Hence clinicians and radiologists must be aware of the characteristic clinical and imaging findings, so as to facilitate timely diagnosis and appropriate multidisciplinary management. Further studies are required for establishing optimal treatment protocols for managing such patients.
- Matos-Miranda C, Nimmo G, Williams B, Tysoe C, Owens M, Bale S, Braverman N: A prospective study of brachytelephalangic Chondrodysplasia punctata: identification of arylsulfatase E mutations, functional analysis of novel missense alleles, and determination of potential phenocopies. Genet Med. 2013, 15:650-7. Available from: https://doi.org/10.1038/gim.2013.13
- Hatia M, Roxo D, Pires MS, Moeda F: Chondrodysplasia punctata: early diagnosis and multidisciplinary management of Conradi-Hünermann-Happle syndrome (CDPX2). Cureus. 2024, 16:e75605. Available from: https://doi.org/10.7759/cureus.75605
- Braverman NE, D'Agostino MD, Maclean GE: Peroxisome biogenesis disorders: biological, clinical and pathophysiological perspectives. Dev Disabil Res Rev. 2013, 17:187-96. Available from: https://doi.org/10.1002/ddrr.1113
- Handa A, Grigelioniene G, Nishimura G: Skeletal dysplasia families: a stepwise approach to diagnosis . Radiographics. 2023, 43:e220067. Available from: https://doi.org/10.1148/rg.220067
- Olarte Bermúdez L, Noguera V, Del Castillo V, et al. (August 24, 2025) Chondrodysplasia punctata: A Rare Entity Identified Incidentally. Cureus 17(8): e90894. Available from: https://doi.org/10.7759/cureus.90894
- Mahale Y, Kadu VV, Chaudhari A: Rare case of rhizomelic Chondrodysplasia punctata . J Orthop Case Rep. 2015, 5:38-40. Available from: https://doi.org/10.13107/jocr.2250-0685.303
- Krakow D. Skeletal dysplasias. Clin Perinatol 2015;42:301‑19, viii
- Krakow D, Rimoin DL: The skeletal dysplasias. Genet Med. 2010, 12:327-41. Available from: https://doi.org/10.1097/GIM.0b013e3181daae9b
- Yalin CT, Bayrak IK, Danaci M, Incesu L: Case report: rhizomelic Chondrodysplasia punctata and foramen magnum stenosis in a newborn (Article in Turkish). Tani Girisim Radyol. 2003, 9:100-3. Available from: https://pubmed.ncbi.nlm.nih.gov/14661305/
- Gerami R, Barkhordari S: Antenatal ultrasonographic diagnosis of rhizomelic Chondrodysplasia punctata . J Ultrasound. 2023, 26:539-42. Available from: https://doi.org/10.1007/s40477-022-00737-5