
More Information
Submitted: March 03, 2026 | Accepted: March 11, 2026 | Published: March 12, 2026
Citation: Riad J, Bajelidze G, Gabos PG. Time to Physeal Closure after Screw Fixation for Slipped Capital Femoral Epiphysis. Arch Clin Exp Orthop. 2026; 10(1): 001-005. Available from:
https://dx.doi.org/10.29328/journal.aceo.1001023
DOI: 10.29328/journal.aceo.1001023
Copyright Licence: © 2026 Riad J, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Slipped capital femoral epiphysis; Physeal closure; Screw fixation; Remodeling

Time to Physeal Closure after Screw Fixation for Slipped Capital Femoral Epiphysis
Jacques Riad1,2*, Gela Bajelidze1 and Peter G Gabos1
1Department of Orthopedics, AI. duPont Hospital for Children Wilmington, Delaware, USA
2Department of Orthopedics, Skaraborg Hospital, Skövde, Institute of Clinical Science, Sahlgrenska Academy, University of Gothenburg, Sweden
*Corresponding author: Jacques Riad, MD, Department of Orthopedics, Skaraborg Hospital, Skövde, Institute of Clinical Science, Sahlgrenska Academy, University of Gothenburg, Sweden, Email: [email protected]
Background: The primary goal of treatment in slipped capital femoral epiphyses (SCFE) is to prevent further slip by stabilizing the physis. This is typically achieved with the use of a single cannulated lag screw placed across the proximal femoral physis to achieve stability and early physeal closure. If screw fixation causes premature physeal closure, it may impact the remodeling potential of the proximal femoral deformity that can occur with SCFE. The influence of this phenomenon on long-term outcome in SCFE is not clear. The goal of this study was to determine the time to physeal closure on the involved and non-involved side after single screw fixation in unilateral SCFE, and to assess factors that may influence this time frame to physeal closure.
Methods: Fifty-two patients with idiopathic unilateral SCFE who had complete radiographs until skeletal maturity were included. Anteroposterior and lateral radiographs of the pelvis and hips were assessed. The position of the screw was noted with attention to the location of the compression threads in relation to the physis and epiphysis, and whether the screw head was flush with the lateral cortex of the femur.
Results: Nineteen girls and 33 boys with a mean age of 11.7 and 14.3 years, respectively, were identified.
Time to closure on the treated side was 8.0 months SD (9,7) (range 0.4 - 52.1) and on the non-involved non-treated side 16.9 months SD (13,5) (range 0.4 - 69.1), which showed a significant difference (p = .001). Ninety-five% confidence interval for the difference was 6,0 - 11,8. Screw position, age, gender, degree of slip, or whether the triradiate cartilage was open or closed did not influence time to closure.
Conclusion: The remaining growth and remodeling potential of the hip after SCFE might be inhibited by the premature closure caused by screw fixation. We speculate that a non-compression device that allows further growth should be used in SCFE for the ultimate long-term outcome.
The primary goal of treatment in Slipped Capital Femoral Epiphyses (SCFE) is to prevent further slip by stabilizing the epiphysis. Whether this should be obtained by an attempt to prematurely close the physis or not is still controversial [1-7].
If the fixation method causes premature physeal closure, it may influence femoral neck growth and remodeling potential of the head-neck deformity, and result in lever arm dysfunction, leg length discrepancy, and impingement and early osteoarthritis [8-10].
By far the most common treatment of SCFE consists of “pinning in situ”, which refers to the application of a single screw or pin across the physis, without reduction of the slip. This provides the best long-term results and decreases the high complication rate that is associated with more extensive early surgical intervention [7,8,11-20].
The most used device is a cannulated compression screw, although the compression aspect of the screw is not always used. Morrissy describes the technique used with one cannulated compression screw [19]. The degree of compression over the physis appears difficult to assess since varying numbers of threads of the screw cross the physis and sometimes are entirely contained in the epiphysis. As well, how flush the screw head is on the lateral cortex of the femur would influence the compression achieved. Studies in vitro have revealed that using compression over the physis yields more than twice as much mechanical compression compared to the non-compression fixation technique [21]. Kumm, et al. describes a dynamic screw fixation technique that provides no compression at all [22,23]. The smooth hook pin device utilized in the Scandinavian countries stabilizes the epiphysis and provides no compression [16].
Recently introduced telescoping screws allow further growth and have the advantage of not protruding laterally in the soft tissue of the proximal femur [24,25].
Remodeling of the proximal femur after SCFE can occur in the metaphysis as a rounding with resorption and apposition of bone [17,26-28]. Physeal remodeling has also been described, where some Investigators report remodeling that ultimately influences the relationship between the head and shaft of the femur [20,29,30]. It is unclear if the consequences of premature closure of the physis would alter this remodeling potential of the proximal femoral deformity that can occur with SCFE, and hence change the outcome of the treatment.
Furthermore, physeal sparing techniques also have implications on prophylactic treatment on the non-slip side at the time of presentation, especially in young patients with a longer time of continued growth, with an increased risk of a contralateral slip and potential significant leg length discrepancy, and provide a secure way of avoiding severe complications such as avascular necrosis [31].
Cousins 2016 observed continued growth, although altered femoral morphology, on the prophylactically treated side using screw fixation with screw threads across the physis [32]. Kumm 2001, using the physeal sparing technique, noted up to 30 mm continued growth on the slip side in mild slips, which was almost as much as on the prophylactically treated non-slip side [22]. Örtegren reported with the Hansson hook pin an increase in femoral neck length, mean 7.1 and 10.0 mm on the slip and prophylactic pinned non-slip side, respectively [10].
Time to closure using screw fixation has not, to our knowledge, been extensively investigated.
The goal of this study was to determine the time to physeal closure with one compression screw on the slip side and compare it to the non-involved and not prophylactically treated contralateral side. Furthermore, to study variables that may influence time to physeal closure.
Approval from the Institutional Review Board was obtained before initiating this retrospective study. Between 1990 and 2002, patients with unilateral SCFE who had screw fixation and complete radiographs were included. Patients with atypical SCFE were excluded. Radiographs were assessed for physeal closure, and the time from the primary surgery until physeal closure was calculated. Closure was defined as 80% or more obliteration of the physis on both the anterior-posterior and lateral view [6]. The date of the first radiograph showing closure was set as the date of closure. If the time interval between the radiograph showing closure and the previous radiograph exceeded 6 months, patients were excluded since the date for closure in these patients was uncertain. Data regarding age, gender, degree of slip, and whether the triradiate cartilage was open or closed were collected. The position of the screw was assessed, and it was noted if the threads of the screw were crossing the physis or were contained entirely within the epiphysis (Figure 1A and B). In addition, the position of the screw head in relation to the lateral cortex was assessed. It was noted if the screw head was flush with the lateral cortex (≤ 5 mm exposure) or left proud (Figure 2A and B). Two orthopedic surgeons who were not involved in the care of any of the patients performed the radiograph assessments.
A two-way analysis of variance was utilized to determine which variables influenced time to physeal closure. Paired samples t-test was used to determine the statistical significance of the time to physeal closure between the SCFE side and the non-involved side.
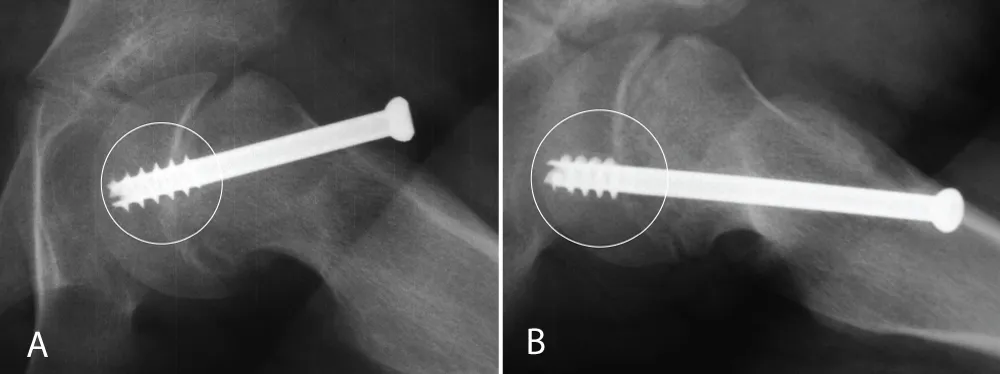
Figure 1: A and B: The threads of the screw crossing the physis, and (1B) the threads of the screw are contained entirely within the epiphysis.

Figure 2: A and B: The screw head is flush with the lateral cortex, and (2B) the screw head is left proud more than 5 mm.
Ninety patients with idiopathic SCFE treated with one cannulated screw in-situ fixation were identified with complete radiographs. Of these, 20 were bilateral, and another 18 went on to develop a contralateral slip later. The remaining 52 patients with unilateral SCFE, followed until skeletal maturity, comprised the study population. Nineteen were girls with a mean age of 11.7 years (range 10.2 - 14.3) and 33 were boys, with a mean age of 14.3 years (range 12.3 - 18.7). The left side was involved in 30 cases and the right side in the remaining 22 cases. The degree of slip according to Southwick was type 1 in 22, type 2 in 16, and type 3 in 14 patients (Southwick 24). Seven cases presented with an unstable SCFE. In 39 cases, the threads of the screw were not all completely across the physis, and in 13 cases, all the screw threads were contained entirely within the epiphysis. In 38 cases, the head of the screw was flush with the lateral cortex, and in 14 it was left proud.
Time to closure on the SCFE side was 8.0 months SD (9,7) (range 0.4 - 52.1) and on the non-involved side it was 16.9 months SD (13,5) (range 0.4 - 69.1). Paired samples t-test was performed and showed a statistically significant difference in time to closure between the SCFE side and the non-involved side (p = .0001) (Table 1).
| Table 1: Mean values and standard deviations in months until physeal closure after unilateral screw fixation of Slipped Capital Femoral Epiphysis. Data for girls, boys, and all children are shown for both the slipped and the non-involved, untreated side. Wilcoxon, non-parametric, signed rank test. | |||
| Time to physeal closure (months) | Significance | ||
| mean and (standard deviations) | p - value | ||
| slip side | non-involved side | ||
| Girls, n = 19 | 9.0 (13.6) | 16.5 (14.6) | <0.001 |
| Boys, n = 33 | 7.5 (6.6) | 17.2 (13.0) | <0.001 |
| All, n = 52 | 8.0 (9.7) | 16.9 (13.5) | <0.001 |
A two-way analysis of variance revealed no significant contributor to differences in time to closure regarding screw positioning, age, gender, degree of slip, or status of the triradiate cartilage. Seven cases had an unstable slip at presentation, and our data did not suggest that the physis in these patients closed earlier or later than the physis in stable slips.
One prevailing theory is that the more remaining growth after surgery for SCFE, the greater the possibility of remodeling, and chances for a good long-term result regarding leg length discrepancy, overgrowth of the greater trochanter, and development of early arthritis. Segal and Edgren reported growth disturbance of the proximal femur in 64% of patients after fixation of juvenile SCFE, including greater trochanter overgrowth, decreased articulo/acetabular trochanteric distance (ATD), coxa vara, and coxa breva [4,33]. Juvenile SCFE was defined as boys 12.5 years or younger and girls 10.5 years or younger in chronological age. Furthermore, an 80% incidence of bilateral involvement was noted, and they recommended a smooth pin construct to allow for further growth, rather than premature closure [4].
Kumm, et al. describe the use of a dynamic screw fixation, where the screw threads are contained in the epiphysis, and the screw head is left proud with 15 to 20 mm lateral to the lateral cortex of the femur [23]. In this way, it was postulated that the physis does not close prematurely, and there is less leg length discrepancy and more time for remodeling. Up to 30 mm continued growth is reported from primary surgery, in mild slips, and in some cases, a second procedure to change to a longer screw is indicated [22,23]. The average time to physeal closure was 3.0 years for boys and 3.2 years for girls. Hansson et al. use a smooth pin with a hook device that leaves room for further growth [16]. Hansson reports femoral neck length growth to be as much as 15 mm after pinning, which is almost as much growth as on the prophylactically pinned non-symptomatic side. Both groups of investigators report that time to closure is similar on both the SCFE side and the prophylactically stabilized side utilizing dynamic techniques [16]. This implies that the fixation technique and device, rather than the disease itself, influence time to closure. Physeal remodeling after SCFE has been described by several authors who found physeal remodeling mainly in moderate and severe slips [20,29,30]. They therefore suggest pinning in situ and then waiting at least two years before considering any realignment procedures of the proximal femur.
Segal, et al. using radiography and computerized tomographic scanning, noted very little remodeling in thirty-eight patients treated with threaded pins [4]. They conclude that although some metaphyseal remodeling occurs, very small changes in the relationship between the femoral head and femoral shaft after pinning in situ for SCFE can be expected. Stanton et al concluded that screw fixation might cause early closure in SCFE [5]. The average time to physeal closure, in their study, was 12 months on the surgically treated side and 22 months on the non-involved, asymptomatic side. They mainly used fully threaded 3 mm pins as compared to one 7.3 mm compression screw used in our series [6]. In 1992, Ward, et al. reported that the position of a single screw and whether the threads of the screw crossed the physis or not influenced the time to closure. The average time to closure was 13 months. There was a significantly shorter time to closure when the screw was placed centrally, rather than in an eccentric position [7]. Jones, et al. describe remodeling and favor pinning in situ and found that those with an open triradiate cartilage remodeled more than those with a closed triradiate cartilage [17]. They anticipated good results with the smooth hook pin described by Hansson 1982.
We found a significant difference in time to closure between the diseased, surgically stabilized side and the non-involved, non-treated side. Whether the difference depends exclusively on the screw fixation or not is still unclear. Our results did not show any differences in time to closure of the physis for variables such as different ways of positioning the screw, the degree of slip, age, or gender.
One of the limitations of this retrospective study is the relatively small number of participants, which limits the wider applicability of the results. Due to the limited imaging and follow-up, we could not assess any possible remodeling or continued growth. The assessment of the screw placement was limited to the positioning of the threads and the head of the screw. Poor consistency in the radiographs and limited imaging made further analysis not possible.
We found an average difference of 9 months in time to physeal closure between the slipped capital femoral epiphysis side and the non-involved side in unilateral SCFE. Neither the position of the screw nor the presence of a stable or unstable slip influenced time to physeal closure. It has previously been shown that continued growth occurs after pinning, and it is reasonable to believe that premature closure influences any remaining remodeling potential. We speculate that a non-compression device that allows further growth should be used in SCFE for the ultimate long-term outcome.
- Chen CE, Ko JY, Wang CJ. Premature closure of the physeal plate after treatment of a slipped capital femoral epiphysis. Chang Gung Med J. 2002;25:811–818. Available from: https://pubmed.ncbi.nlm.nih.gov/12635837/
- Herndon CH, Heyman CH, Bell DM. Treatment of slipped capital femoral epiphysis by epiphyseodesis and osteoplasty of the femoral neck: a report of further experiences. J Bone Joint Surg Am. 1963;45:999–1012. Available from: https://pubmed.ncbi.nlm.nih.gov/14046478/
- Melby A, Hoyt WA Jr, Weiner DS. Treatment of chronic slipped capital femoral epiphysis by bone-grafted epiphyseodesis. J Bone Joint Surg Am. 1980;62:119–125. Available from: https://pubmed.ncbi.nlm.nih.gov/6985910/
- Segal LS, Davidson RS, Robertson WW Jr, Drummond DS. Growth disturbances of the proximal femur after pinning of juvenile slipped capital femoral epiphysis. J Pediatr Orthop. 1991;11:631–637. Available from: https://pubmed.ncbi.nlm.nih.gov/1918351/
- Southwick WO. Osteotomy through the lesser trochanter for slipped capital femoral epiphysis. J Bone Joint Surg Am. 1967;49:807–835. Available from: https://pubmed.ncbi.nlm.nih.gov/6029256/
- Stanton RP, Shelton YA. Closure of the physis after pinning of slipped capital femoral epiphysis. Orthopedics. 1993;16:1099–1102; discussion 1102–1103. Available from: https://doi.org/10.3928/0147-7447-19931001-04
- Ward WT, Stefko J, Wood KB, Stanitski CL. Fixation with a single screw for slipped capital femoral epiphysis. J Bone Joint Surg Am. 1992;74:799–809. Available from: https://pubmed.ncbi.nlm.nih.gov/1634570/
- Hagglund G, Hansson LI, Ordeberg G, Sandstrom S. Slipped capital femoral epiphysis in southern Sweden: long-term results after femoral neck osteotomy. Clin Orthop Relat Res. 1986:152–159. Available from: https://doi.org/10.3109/17453678709154165
- Helgesson L, Kälebo P, Johansson Aurell Y, Tiderius CJ, Kärrholm J, Riad J. Early osteoarthritis after slipped capital femoral epiphysis. Acta Orthop. 2018;89(2):222–228. Available from: https://doi.org/10.1080/17453674.2017.1407055
- Örtegren J, Björklund-Sand L, Engbom M, Siversson C, Tiderius CJ. Unthreaded fixation of slipped capital femoral epiphysis leads to continued growth of the femoral neck. J Pediatr Orthop. 2016 Jul–Aug;36(5):494–498. Available from: https://doi.org/10.1097/bpo.0000000000000684
- Aronson DD, Carlson WE. Slipped capital femoral epiphysis: a prospective study of fixation with a single screw. J Bone Joint Surg Am. 1992;74:810–819. Available from: https://pubmed.ncbi.nlm.nih.gov/1634571/
- Aronson DD, Peterson DA, Miller DV. Slipped capital femoral epiphysis: the case for internal fixation in situ. Clin Orthop Relat Res. 1992:115–122. Available from: https://pubmed.ncbi.nlm.nih.gov/1499197/
- Boyer DW, Mickelson MR, Ponseti IV. Slipped capital femoral epiphysis: long-term follow-up study of one hundred and twenty-one patients. J Bone Joint Surg Am. 1981;63:85–95. Available from: https://pubmed.ncbi.nlm.nih.gov/7451529/
- Carney BT, Weinstein SL, Noble J. Long-term follow-up of slipped capital femoral epiphysis. J Bone Joint Surg Am. 1991;73:667–674. Available from: https://pubmed.ncbi.nlm.nih.gov/2045391/
- Emery RJ, Todd RC, Dunn DM. Prophylactic pinning in slipped upper femoral epiphysis: prevention of complications. J Bone Joint Surg Br. 1990;72:217–219. Available from: https://doi.org/10.1302/0301-620x.72b2.2312558
- Hansson LI. Osteosynthesis with the hook-pin in slipped capital femoral epiphysis. Acta Orthop Scand. 1982;53:87–96. Available from: https://doi.org/10.3109/17453678208992184
- Jones JR, Paterson DC, Hillier TM, Foster BK. Remodelling after pinning for slipped capital femoral epiphysis. J Bone Joint Surg Br. 1990;72:568–573. Available from: https://doi.org/10.1302/0301-620x.72b4.2380205
- Morrissy RT. In situ fixation of chronic slipped capital femoral epiphysis. Instr Course Lect. 1984;33:319–327. Available from: https://pubmed.ncbi.nlm.nih.gov/2703717/
- Morrissy RT. Slipped capital femoral epiphysis: technique of percutaneous in situ fixation. J Pediatr Orthop. 1990;10:347–350. Available from: https://doi.org/10.1097/01241398-199005000-00010
- Wong-Chung J, Strong ML. Physeal remodeling after internal fixation of slipped capital femoral epiphyses. J Pediatr Orthop. 1991;11:2–5. Available from: https://doi.org/10.1097/01241398-199101000-00002
- Early SD, Hedman TP, Reynolds RA. Biomechanical analysis of compression screw fixation versus standard in situ pinning in slipped capital femoral epiphysis. J Pediatr Orthop. 2001;21:183–188. Available from: https://pubmed.ncbi.nlm.nih.gov/11242247/
- Kumm DA, Lee SH, Hackenbroch MH, Rutt J. Slipped capital femoral epiphysis: a prospective study of dynamic screw fixation. Clin Orthop Relat Res. 2001:198–207.
- Kumm DA, Schmidt J, Eisenburger SH, Rutt J, Hackenbroch MH. Prophylactic dynamic screw fixation of the asymptomatic hip in slipped capital femoral epiphysis. J Pediatr Orthop. 1996;16:249–253. Available from: https://doi.org/10.1097/00004694-199603000-00023
- Leblanc E, Bellemore JM, Cheng T, Little DG, Birke O. Biomechanical considerations in slipped capital femoral epiphysis and insights into prophylactic fixation. J Child Orthop. 2017;11:120–127. Available from: https://doi.org/10.1302/1863-2548-11-170012
- Morash K, Orlik B, El-Hawary R, Gauthier L, Logan K. Femoral neck growth and remodeling with free-gliding screw fixation of slipped capital femoral epiphysis. J Pediatr Orthop. 2021;41(4):e309–e315. Available from: https://doi.org/10.1097/bpo.0000000000001770
- Clarke NM, Harrison MH. Slipped upper femoral epiphysis: a potential for spontaneous recovery. J Bone Joint Surg Br. 1986;68:541–544. Available from: https://doi.org/10.1302/0301-620x.68b4.3733827
- Kallio PE, Foster BK, LeQuesne GW, Paterson DC. Remodeling in slipped capital femoral epiphysis: sonographic assessment after pinning. J Pediatr Orthop. 1992;12:438–443. Available from: https://doi.org/10.1097/01241398-199207000-00004
- O'Brien ET, Fahey JJ. Remodeling of the femoral neck after in situ pinning for slipped capital femoral epiphysis. J Bone Joint Surg Am. 1977;59:62–68. Available from: https://pubmed.ncbi.nlm.nih.gov/833177/
- Radlo W, Felus J, Kotulski D. Clinical outcome and assessment of spontaneous remodeling of slipping angle in SCFE. Chir Narzadow Ruchu Ortop Pol. 2004;69:373–378.
- Sibinski M, Snyder M, Borowski A, Grzegorzewski A. Remodeling after in situ pinning for slipped capital femoral epiphysis. Chir Narzadow Ruchu Ortop Pol. 2004;69:321–324. Available from: https://pubmed.ncbi.nlm.nih.gov/15751721/
- Ibrahim T, Ball M, Riaz M, Kenawey MJ. Avascular necrosis and time to surgery for unstable slipped capital femoral epiphysis: a systematic review and meta-analysis. J Pediatr Orthop. 2022 Nov–Dec;42(10):545–551. Available from: https://doi.org/10.1097/bpo.0000000000002179
- Cousins GR, Campbell DM, Wilson NL, Maclean JGB. Prophylactic pinning for slipped capital femoral epiphysis: does it affect proximal femoral morphology? J Pediatr Orthop B. 2016;25:202–206. Available from: https://doi.org/10.1097/bpb.0000000000000252
- Edgren W. Coxa plana: a clinical and radiological investigation with particular reference to the importance of the metaphyseal changes for the final shape of the proximal part of the femur. Acta Orthop Scand Suppl. 1965;84:1–129. Available from: https://pubmed.ncbi.nlm.nih.gov/5850148/